Mental Health First Aid Standard Reference Guide
Can Anyone Help My Mind?
The artist is in the middle of a crowd and feeling envious that other people have such full lives with work, families and happiness. He feels like an outcast. All the faces look the same because the artist was reflecting his desire to fit in and be like everyone else.
Welcome to Mental Health First Aid (MHFA)
In any given year, one in five people in Canada are living with a mental health or substance use problem (Mental Health Commission of Canada, 2013; Smetanin et al., 2011). Some mental health and substance use problems are more common than many physical health problems. While people often know a lot about physical illness, most people have little knowledge about mental illness. This lack of understanding promotes fear and stigma. It prevents people from seeking help early and from seeking the most effective help. It also keeps people from providing support to friends, colleagues, family members and people around them simply because they do not know how.
Our mental health (also referred to as mental wellness or well-being) allows us to realize our potential, cope with stress effectively, bounce back from life challenges and be active, productive members of our communities. How each of us defines our mental health/wellness/well-being can be very different and quite individualized, it is about living well and feeling capable despite life’s challenges (Minister of Public Works and Government Services Canada, 2006).
Note: In this MHFA course, we’ll use the term “mental well-being.”
The Mental Health First Aid (MHFA) training course was developed to help people provide initial support to someone who may be experiencing a decline in their mental well-being or may be in crisis. The philosophy behind MHFA is that mental health and substance use crises, such as suicidal and self-harming actions, may be avoided through early intervention. If crises do arise, then members of the public can take action that may reduce the harm that could result.
Course participants will learn how to recognize the range of changes that may be a sign of declining mental well-being or crisis, how to offer and to provide help, and how to guide a person towards appropriate treatments and supports.
This guide has been developed to accompany the MHFA Canada course. The “Contents” page provides a snapshot of the topics addressed. Please note that the contents of this guide, including all wording, graphics, images and other material, are not intended to replace consultations with a family physician or professional, or to provide medical advice, diagnosis or treatment. Don’t use this information to diagnose or develop a treatment plan for a mental health or substance use problem without consulting a qualified health care provider.
We appreciate your interest in supporting others who may be experiencing mental distress. And, we encourage you to use what you’ll learn for your own mental well-being.
Enjoy the course!
Source: Paintings in this document
The painting on the front cover, along with the paintings at the beginning of sections 1, 2.1, 2.2 and 2.3, were reproduced with permission from the “Out of the Shadows” artist’s program in Edmonton, which offers community arts opportunities to individuals living with mental health concerns. The artist wishes to remain anonymous.
© 2024 Mental Health Commission of Canada. All rights reserved. This material is protected by copyright laws internationally in over 200 countries. Permission to use this publication is granted strictly for personal, non-commercial use. No part of this publication may be modified, translated, reproduced, publicly displayed, stored in a retrieval system, uploaded to a website, or be distributed or transmitted in any form by any means whatsoever, whether electronic, mechanical, recording, or otherwise, without the explicit written authorization of the Mental Health Commission of Canada. Modification, translation, reproduction, public display, transmission or distribution of this publication, in whole or part, is a violation of copyright and may result in legal action as well as criminal penalties.
Disclaimer
The information provided in this course is for mental health and substance use first aid use only and is not intended to be and should not be relied upon as a substitute for professional mental health and substance use advice.
Mental Health Commission of Canada and Opening Minds
MHFA Program
Acknowledgements
Section 1: Introduction to MHFA

Real and Unreal
The artist is constantly shifting between his real world and his unreal world. He goes back and forth and sometimes loses touch with what is real and what is unreal. Sometimes he feels he may not really exist. Space and time disappear.
Welcome to Mental Health First Aid
In any given year, one in five people in Canada are living with a mental health or substance use problem (Mental Health Commission of Canada, 2013; Smetanin et al., 2011). Some mental health and substance use problems are more common than many physical health problems. While people often know a lot about physical illness, most people have little knowledge about mental illness. This lack of understanding promotes fear and stigma. It prevents people from seeking help early and from seeking the most effective help. It also keeps people from providing support to friends, colleagues, family members and people around them simply because they do not know how.
Our mental health (also referred to as mental wellness or well-being) allows us to realize our potential, cope with stress effectively, bounce back from life challenges and be active, productive members of our communities. How each of us defines our mental health/wellness/well-being can be very different and quite individualized, it is about living well and feeling capable despite life’s challenges (Minister of Public Works and Government Services Canada, 2006).
Note: In this MHFA course, we’ll use the term “mental well-being.”
The Mental Health First Aid (MHFA) training course was developed to help people provide initial support to someone who may be experiencing a decline in their mental well-being or may be in crisis. The philosophy behind MHFA is that mental health and substance use crises, such as suicidal and self-harming actions, may be avoided through early intervention. If crises do arise, then members of the public can take action that may reduce the harm that could result.
Course participants will learn how to recognize the range of changes that may be a sign of declining mental well-being or crisis, how to offer and to provide help, and how to guide a person towards appropriate treatments and supports.
This guide has been developed to accompany the MHFA Canada course. The “Contents” page provides a snapshot of the topics addressed. Please note that the contents of this guide, including all wording, graphics, images and other material, are not intended to replace consultations with a family physician or professional, or to provide medical advice, diagnosis or treatment. Don’t use this information to diagnose or develop a treatment plan for a mental health or substance use problem without consulting a qualified health care provider.
We appreciate your interest in supporting others who may be experiencing mental distress. And, we encourage you to use what you’ll learn for your own mental well-being.
Enjoy the course!
Background
Who We Are
Opening Minds
Created in 2023 as a stand-alone not-for-profit organization, Opening Minds is a social enterprise operating alongside the Mental Health Commission of Canada with a focus on providing training programs such as Mental Health First Aid (MHFA), The Working Mind (TWM), and The Inquiring Mind (TIM). These programs seek to change Canadians’ behaviours and attitudes toward people living with mental health and substance use problems and illnesses, helping to ensure people are treated fairly and as full citizens with opportunities to contribute to society like anyone else.
Opening Minds‘ mission is to be the leader of evidence-based programs that promote mental health, well-being, and resilience, and eliminate stigma around the world.
Mental Health Commission of Canada
The Mental Health Commission of Canada (MHCC) is a charity created to focus national attention on mental health issues and to work to improve the health and social outcomes of people living with mental health and substance use problems and illnesses. MHCC leads the development and dissemination of innovative programs and tools to support Canadians’ mental health and well-being.
Through its unique mandate from the Government of Canada, the MHCC supports federal, provincial and territorial governments, and organizations in implementing sound public policy.
Each of MHCC’s initiatives and projects is led by experts from across the country who bring a range of experience and a variety of perspectives to the table. Consulting with people who have experience living with a
mental health or substance use problem as well as their families is a key aspect in all of the MHCC’s work. This work includes offering a host of resources, tools and training programs aimed at increasing mental health and substance use literacy and improving the mental well-being of all people living in Canada.
MHFA Program
This program is run by MHFA International, trading as Mental Health First Aid Australia, which is a not-for-profit company. MHFA training has been licenced to operate in numerous countries: Bermuda, Canada, Denmark, England, Finland, Hong Kong, India, Ireland, Japan, Malta, Nepal, Netherlands, New Zealand, Northern Ireland, Pakistan, Saudi Arabia, Scotland, Singapore, Sweden, UAE, USA and Wales. When the MHFA Program was adopted in these countries, either a mental health government agency or a nongovernment mental health organization tailored the MHFA Australia course materials to their own culture and health care system and worked out the method of dissemination best suited to local conditions. The MHFA Canada program came under the leadership of the Mental Commission of Canada (MHCC) in February 2010 and Opening Minds in 2023.
An important factor in the MHFA Program’s international spread has been the continuing attention to research and evaluation. The MHFA course has been thoroughly evaluated using randomized controlled trials and a qualitative study and been found to be effective at:
Improving course participants’ knowledge of mental health and substance use problems
Reducing stigma
Increasing the amount of help provided to others
Acknowledgements
The MHFA course was originally developed in Canberra by Betty Kitchener, an educator and mental health consumer, in partnership with Professor Tony Jorm, a mental health researcher. The aim in creating the program
was to extend the concept of first aid training to include mental health and substance
use problems so that community members were empowered to provide better initial support to someone who is developing a mental health and/or substance use problem, has experienced a worsening of an existing mental health and/or substance use problem, or is in a mental health and/or substance use crisis.
The first aid information in this Reference Guide is based on guidelines developed by the Australian Mental Health First Aid®
Training and Research Program from 2006 to 2008, using the consensus of international expert panels involving mental health and substance use consumers, caregivers and professionals. The following people worked on the development of these guidelines: Claire Kelly, Robyn Langlands, Anna Kingston and Laura Hart. Further details of the guidelines may be found at www.mhfa.com.au.
The Canadian edition was compiled by the Mental Health Commission of Canada (MHCC) and reviewed by experts in mental health and substance use disorders. This reference guide is based on the Australian version, referred to as “MHFA Manual, version 4.” Content was modified, adapted and edited for Canada.
Opening Minds thanks the following people who were involved in the development of the original version of the course from which this updated version was developed:
Dr. Doug Watson (Alberta Health Services),
Dr. Roger Bland (University of Alberta),
Dr. Stephen Newman (University of Alberta),
Dr. Scott B. Patten (University of Calgary),
Betty Kitchener (MHFA Australia),
Dr. Anthony Jorm (MHFA Australia),
Julie Peacock (Alberta Health Services),
Richard Ramsay (LivingWorks),
MHFA Canada instructors Karen Kyliuk, Anthony Prime, Marion Cooper, John Mitchell and Yvonne Walsh for providing feedback
ALMIER for permission to reproduce his artwork. Artwork was provided through the “Out of the Shadows” artists’ program, which offers community arts opportunities to individuals living with mental health and substance use concerns in Alberta’s Capital Health region.
Mental Health and Substance Use Problems in Canada
What is mental health?
There are different ways of defining the term “mental health.” Some definitions emphasize positive psychological well-being, whereas others see it as the absence of mental health and substance use problems.
For example, the World Health Organization has defined “mental health” as:
“…a state of well-being in which the individual realizes his or her own abilities, can cope with the normal stresses of life, can work productively, and is able to make a contribution to his or her community”
(World Health Organization, 2018)
For many, mental health also incorporates a spiritual dimension along with the physical, mental and social aspects of wellness. Mental health influences how we think and feel about ourselves and others and how we interpret events. It affects our capacity to learn, communicate, and form, sustain or end relationships. Good mental health buffers us from stresses and hardships that are part of life for us all. It can help reduce the risk of developing mental health and substance use problems or disorders. Even when someone develops a problem or disorder, they can nonetheless experience good mental health, and this can contribute to their journey of recovery (Provencher & Keyes, 2011).
Mental well-being or mental wellness
These two terms are often used interchange- ably with mental health when referring to positive mental health. Our mental health/wellness/well-being allows us to realize our potential, cope with stress effectively, bounce back from life challenges and be active, productive members of our communities.
How each of us defines our mental health/ wellness/well-being can be very different and quite individualized. It is about living well and feeling capable despite life’s challenges (Canadian Mental Health Association, 2014).
Note: In this MHFA course, we’ll use the term “mental well-being.”
What are mental health disorders?
A mental disorder or mental illness is a diagnosable illness that affects a person’s thinking, emotional state and behaviour, and disrupts the person’s ability to work or
carry out other daily activities and engage in satisfying personal relationships (American Psychiatric Association, 2013).
Some people have only one episode of mental illness in their lifetime, while others have multiple episodes and periods of wellness in between. Only a small minority have ongoing mental health problems.
There are different types of mental illnesses, some of which are common, such as depression and anxiety disorders, and some which are not common, such as schizophrenia and bipolar disorder. However, mental illnesses, as with any health problem, cause disability, which is sometimes severe. In Canada, most health professionals will use the Diagnostic Statistical Manual 5 (DSM 5)
or International Classification of Diseases (ICD 10) to determine whether or not a person meets the criteria for diagnosis of a mental disorder.
Concurrent Disorders
(Centre for Addiction and Mental Health, n.d.-a)
Mental health problems can often occur in combination with substance use or addiction disorder. Research shows that more than 50% of those seeking help for a substance use disorder or addiction also have a mental illness, and 15-20% of those seeking help from mental health services are also living with an addiction or substance use disorder (Centre for Addiction and Mental Health, n.d.-a).
Concurrent disorders is a term used to refer to co-occurring addiction and mental health problems. This term covers a wide array of combinations of problems, such as: anxiety disorder and an alcohol problem, schizophrenia and cannabis dependence, borderline personality disorder and heroin dependence, and bipolar disorder and problem gambling. These problems can
co-occur in a variety of ways. They may be active at the same time or at different times, in the present or in the past, and their symptoms may vary in intensity and form over time. People often ask, “Which came first: the mental health problem or the substance use problem?” This is a hard
question to answer. It’s more useful to think of them as independent problems that interact with each other.
What are “problems”?
A mental health or substance use problem is a broader term including both mental health- and substance use-related illnesses and symptoms that may not be severe enough to warrant the diagnosis of a disorder.
A variety of terms are used to describe mental health and substance use problems: mental illness, mental ill-health, mental health and substance use condition, psychiatric illness, nervous exhaustion, mental breakdown, nervous breakdown and burnout. Slang terms such as crazy, psycho, mad, loony, nuts, cracked-up and wacko promote stigmatizing attitudes and should not be used.
These terms do not give much information about what the person is really experiencing. Worse, slang terms reinforce negative attitudes about mental health and substance use problems and can be hurtful. Myths, misinformation and lack of knowledge lead to stigma around mental health and substance use problems and discrimination that prevents people from accessing help and hinders recovery.
This guide provides information on how to assist people with mental health and
substance use problems and not only those with diagnosable disorders. There are so many different types that it is not possible to cover them all in this guide. The most common problems, as well as the most severe problems, are covered. However, it is important to note that the MHFA principles in this guide can be usefully applied to other mental health and substance use problems.
Why is MHFA Needed?
There are many reasons why people need training in MHFA.
Mental health and substance problems are common
Over the course of any person’s life, it is highly likely that they will develop a mental health or substance use problem themselves or have close contact with someone who does. In any given year, one in five people in Canada are living with a mental health or substance use problem or illness (Mental Health Commission of Canada, 2013; Smetanin et al., 2011).
However, there are many people that do not reach out for help. Others seek help from sources that are not tracked by statistics, such as private therapy. Mental health and substance use problems are a common reason for people consulting their physician.
Over 1 million Canadians with a mental health-related disability say they require counselling services from a psychologist, psychiatrist, psychotherapist, or social
worker (Statistics Canada, 2019). These results reflect the general population. Research on subpopulations may show higher or lower rates of mental health and substance use problems. For example, the rate of mental illness in prisons is
4 to 7 times higher than in the general community (Centre for Addiction and Mental Health, n.d.-b). A 2016 study reported that 44% of newly admitted male offenders in federal correctional system
in Canada met the criteria for anxiety disorders and 49% met the criteria for substance use disorders (Beaudette & Stewart, 2016).
| ESTIMATED 12-MONTH PREVALENCE OF ANY MENTAL ILLNESS IN CANADA, 2011 | ||
|---|---|---|
|
|
Total Number of People |
Percentage of the Population |
|
ALL MAJOR DISORDERS (not including childhood disorders, such as ADHD) |
6,797,627 |
19.8% |
|
MOOD AND ANXIETY-RELATED DISORDERS |
4,016,700 |
11.75% |
|
SUBSTANCE USE DISORDERS |
2,029,200 |
5.9% |
|
COGNITIVE IMPAIRMENT & DEMENTIAS |
747, 100 |
2.17% |
|
SCHIZOPHRENIA |
210,540 |
0.61% |
Figure 1: Estimated 12-Month Prevalence of Any Mental Health Illness in Canada (Mental Health Commission of Canada, 2013; Smetanin et al., 2011)
Professional help is not always on hand
Family physicians, counsellors, psychologists, psychiatrists and other
professionals can all assist people with mental health and substance use
problems. However, as with injuries and other medical emergencies, such
assistance is not always available when a problem first arises. This is when members of the public who are trained in MHFA can offer immediate aid and support the person until appropriate professional help is received.
Members of the general public often do not know how to respond
Even in an emergency, a person wishing to give assistance at a motor vehicle crash may be reluctant to help for fear of doing the “wrong thing.” Similarly, in a mental health and substance use situation, the first aider’s actions may determine how quickly the person with the problem gets help and/or recovers. In any first aid course, participants learn how to help someone who is injured or ill. The first aider learns how to remain calm and confident and to respond in an appropriate way to give the best help until the crisis is resolved or professional help is obtained.
There is stigma associated with mental health and substance use problems
Stigma refers to negative attitudes (prejudice) and negative behaviour (discrimination) toward people with mental health and substance use problems. Stigma means having fixed ideas and judgments about people, as well as fearing and avoiding what we don’t understand (Centre for Addiction and Mental Health, 2007).
The stigma attached to mental health and substance use problems presents a serious barrier to assessment, diagnosis, treatment and support needed for recovery as well as acceptance in the community (Minister of Public Works and Government Services Canada, 2006).
Stigma results in the exclusion of people with mental health and substance use problems from activities that are open to other people, such as getting a job, finding a safe place to live, participating in social activities and having relationships (Centre for Addiction and Mental Health, 2007).
The prejudice and discrimination they face often becomes internalized. They begin to believe the negative things that other people and the media say about them (self-stigma) and they have lower self-esteem because they feel guilt and shame. As a result, they often do not seek the help they need (Centre for Addiction and Mental Health, 2007).
In fact, a Health Canada survey reported that 54 per cent of respondents (who met the criteria for anxiety-related disorder, mood-related disorder or substance dependence) felt embarrassed about their mental health and substance use problems, and 54 per cent reported facing discrimination for their mental health and substance use problems. Not everyone with a mental health or substance use problem seeks treatment (Minister of Public Works and Government Services Canada, 2006).
Not all mental health and substance use problems require professional help. However, people who do require treatment may not seek professional help for a variety of reasons, such as an inability to recognize their mental health and substance use problems, a lack of health professionals, or a lack of knowledge about what services are available. According to the Canadian Community Healthcare Survey (2012), only 10.5 per cent of all respondents who had experienced a mental health disorder, or a substance dependency problem said they had accessed a professional consultation or used services in the 12 months preceding the study (Statistics Canada, 2012).
People may lack the insight to realize that they need help or that help is available. Some mental health and substance use problems cloud clear thinking and good decision-making. A person experiencing such problems may not realize that they need help or that effective help is available. They may be in such a state of distress that they are unable to think clearly about what they should do.
Many people are not well informed
Although the general public’s knowledge about mental health and substance use problems is slowly improving, there is still a widespread lack of understanding about how to recognize these problems and what effective treatments are available (Jorm et al., 1997).
There are many myths about mental health and substance use problems, such as people that live with these problems are violent, that they can make themselves better if they wanted to or that these problems are contagious. As a result, people may not know when or where to seek help or what kind of help might be useful.
With greater community awareness, people will be able to recognize their own problems, or those of others, and feel more comfortable about seeking professional help.
There are many reasons why people need training in MHFA.
1. Mental health and substance problems are common
Over the course of any person’s life, it is highly likely that they will develop a mental health or substance use problem themselves or have close contact with someone who does. In any given year, one in five people in Canada are living with a mental health or substance use problem or illness (Mental Health Commission of Canada, 2013; Smetanin et al., 2011).
However, there are many people that do not reach out for help. Others seek help from sources that are not tracked by statistics, such as private therapy. Mental health and substance use problems are a common reason for people consulting their physician.
Over 1 million Canadians with a mental health-related disability say they require counselling services from a psychologist, psychiatrist, psychotherapist, or social
worker (Statistics Canada, 2019). These results reflect the general population. Research on subpopulations may show higher or lower rates of mental health and substance use problems. For example, the rate of mental illness in prisons is
4 to 7 times higher than in the general community (Centre for Addiction and Mental Health, n.d.-b). A 2016 study reported that 44% of newly admitted male offenders in federal correctional system
in Canada met the criteria for anxiety disorders and 49% met the criteria for substance use disorders (Beaudette & Stewart, 2016).
| ESTIMATED 12-MONTH PREVALENCE OF ANY MENTAL ILLNESS IN CANADA, 2011 | ||
|---|---|---|
|
|
Total Number of People |
Percentage of the Population |
|
ALL MAJOR DISORDERS (not including childhood disorders, such as ADHD) |
6,797,627 |
19.8% |
|
MOOD AND ANXIETY-RELATED DISORDERS |
4,016,700 |
11.75% |
|
SUBSTANCE USE DISORDERS |
2,029,200 |
5.9% |
|
COGNITIVE IMPAIRMENT & DEMENTIAS |
747, 100 |
2.17% |
|
SCHIZOPHRENIA |
210,540 |
0.61% |
Figure 1: Estimated 12-Month Prevalence of Any Mental Health Illness in Canada (Mental Health Commission of Canada, 2013; Smetanin et al., 2011)
2. Professional help is not always on hand
Family physicians, counsellors, psychologists, psychiatrists and other
professionals can all assist people with mental health and substance use
problems. However, as with injuries and other medical emergencies, such
assistance is not always available when a problem first arises. This is when members of the public who are trained in MHFA can offer immediate aid and support the person until appropriate professional help is received.
3. Members of the general public often do not know how to respond
Even in an emergency, a person wishing to give assistance at a motor vehicle crash may be reluctant to help for fear of doing the “wrong thing.” Similarly, in a mental health and substance use situation, the first aider’s actions may determine how quickly the person with the problem gets help and/or recovers. In any first aid course, participants learn how to help someone who is injured or ill. The first aider learns how to remain calm and confident and to respond in an appropriate way to give the best help until the crisis is resolved or professional help is obtained.
4. There is stigma associated with mental health and substance use problems
Stigma refers to negative attitudes (prejudice) and negative behaviour (discrimination) toward people with mental health and substance use problems. Stigma means having fixed ideas and judgments about people, as well as fearing and avoiding what we don’t understand (Centre for Addiction and Mental Health, 2007).
The stigma attached to mental health and substance use problems presents a serious barrier to assessment, diagnosis, treatment and support needed for recovery as well as acceptance in the community (Minister of Public Works and Government Services Canada, 2006).
Stigma results in the exclusion of people with mental health and substance use problems from activities that are open to other people, such as getting a job, finding a safe place to live, participating in social activities and having relationships (Centre for Addiction and Mental Health, 2007).
The prejudice and discrimination they face often becomes internalized. They begin to believe the negative things that other people and the media say about them (self-stigma) and they have lower self-esteem because they feel guilt and shame. As a result, they often do not seek the help they need (Centre for Addiction and Mental Health, 2007).
In fact, a Health Canada survey reported that 54 per cent of respondents (who met the criteria for anxiety-related disorder, mood-related disorder or substance dependence) felt embarrassed about their mental health and substance use problems, and 54 per cent reported facing discrimination for their mental health and substance use problems. Not everyone with a mental health or substance use problem seeks treatment (Minister of Public Works and Government Services Canada, 2006).
Not all mental health and substance use problems require professional help. However, people who do require treatment may not seek professional help for a variety of reasons, such as an inability to recognize their mental health and substance use problems, a lack of health professionals, or a lack of knowledge about what services are available. According to the Canadian Community Healthcare Survey (2012), only 10.5 per cent of all respondents who had experienced a mental health disorder, or a substance dependency problem said they had accessed a professional consultation or used services in the 12 months preceding the study (Statistics Canada, 2012).
People may lack the insight to realize that they need help or that help is available. Some mental health and substance use problems cloud clear thinking and good decision-making. A person experiencing such problems may not realize that they need help or that effective help is available. They may be in such a state of distress that they are unable to think clearly about what they should do.
5. Many people are not well informed
Although the general public’s knowledge about mental health and substance use problems is slowly improving, there is still a widespread lack of understanding about how to recognize these problems and what effective treatments are available (Jorm et al., 1997).
There are many myths about mental health and substance use problems, such as people that live with these problems are violent, that they can make themselves better if they wanted to or that these problems are contagious. As a result, people may not know when or where to seek help or what kind of help might be useful.
With greater community awareness, people will be able to recognize their own problems, or those of others, and feel more comfortable about seeking professional help.
Impacts
How disabling are mental health and substance use problems?
Mental health and substance use problems can be more disabling for a person than many chronic physical illnesses. “Disability” refers to the amount of disruption that a health problem causes to a person’s ability to work, look after themselves and carry on their relationships with family and friends.
Research in the Netherlands has looked at the amount of disability caused by a large number of both physical and mental health and substance use problems (Stouthard et al., 1997). It helps to understand the amount of disability that mental health and substance
use problems can cause by comparing them to physical health problems that cause the same amount of disability. Here are some examples:
- The disability caused by moderate depression is similar to the disability from relapsing multiple sclerosis, severe asthma, chronic hepatitis B or deafness.
- The disability from severe post-traumatic stress disorder is comparable to the disability from paraplegia.
- The disability from severe schizophrenia is comparable to the disability from quadriplegia.
Global Burden of Disease studies have highlighted mental and substance use disorders as the leading cause of disability globally (Whiteford et al., 2016), and The World Health Organization (2019) described how mental, neurological, and substance use disorders make up 10 % of the global burden of disease and 30% of the non-fatal disease burden.
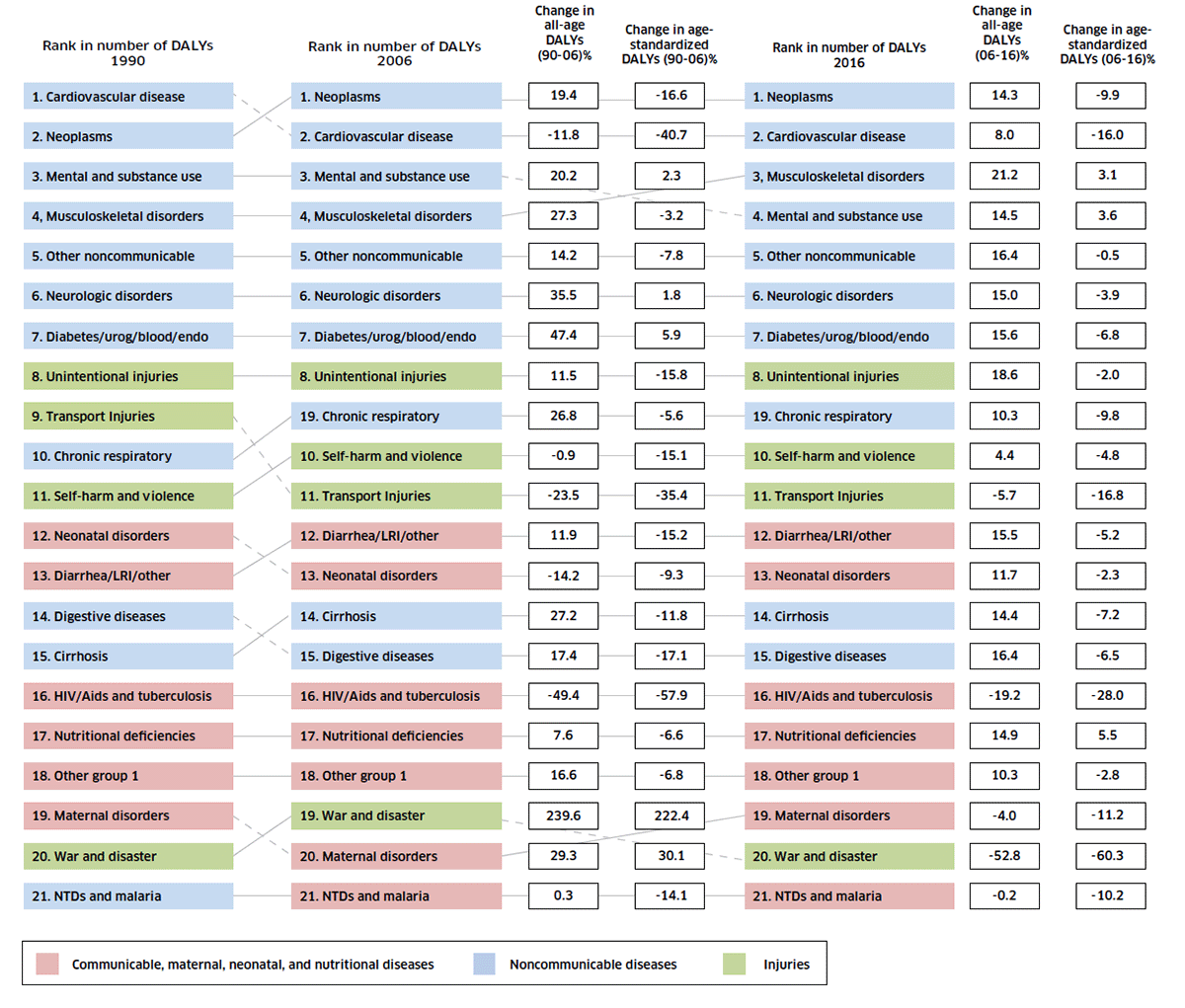
The graph below (Figure 2) shows the burden of disease in Canada, as measured by Disability Adjusted Life Years (DALY). DALY combines years lost due to premature death and years lived with a disability. Between 1990-2006 “mental and substance use” in Canada ranked third and more recently was ranked fourth in 2016 behind neoplasms (cancer), cardiovascular diseases, and mus- culoskeletal diseases (Lang et al., 2018). In Canada, mental and behavioural disorders account for 23% of years of life lost due to disability and 13% of years of life lost due
to disability and premature mortality (Public Health Agency of Canada, 2015). Higher mortality rates due to opioid-related mortality in Canada have contributed to increases in burden of disease measurements (Public Health Agency of Canada, 2015).
Impact of mental health and substance use problems
Mental health and substance use problems affect people of all ages, cultures, and education and income levels. “Mental illnesses have the potential to impact every aspect of an individual’s life, including relationships, education, work, and community involvement” (Public Health Agency of Canada, 2015. p.3).
They also indirectly affect all Canadians through illness in a family member, friend or colleague, and they are costly to the individual, their family, the health care system and the community.
It is important to realize that many mental health and substance use problems are time limited and people are able to take up their lives as before. Even when people experience more serious, long-term or recurring problems, they are still able to live meaningful and satisfying lives. This may mean making some adjustments to accommodate the effects of their mental health and substance use problem.
Examples of the impact of mental health and substance use problems
- Every week at least 500,000 Canadians miss work due to mental illness. The annual economic burden of mental illness in Canada is estimated to be $51 billion. By 2041, the cumulative cost of poor mental health to the Canadian economy is estimated to exceed $2.5 trillion (Centre for Addiction and Mental Health, 2020).
- A 2017 survey of the Canadian workforce, found that 78% of respondents missed work due to mental health problems and illnesses and 34% of those missing work, were away from work for two or more months (Morneau Shepell, 2017).
- A 2019 report on Canadian mental health in the workplace listed on average 30% of short-term claims and 43% of long-term claims were due to mental health diagnoses (Deloitte, 2019).
- Additionally, a survey of organizations that operate in all major industry sections found depression, anxiety, and stress to be the primary cause of mental illness-related disability claims in Canada (Public Health Agency of Canada, 2015).
- Based on the 2017 Canadian Survey on Disability, the employment rate among people with a mental health-related disability was 46%, compared with approximately 80% for people without a disability. Over half of those with a mental health-related disability believed they were disadvantaged in employment because of their condition (Statistics Canada, 2020).
- Aside from the impact on individuals, society also bears the costs of mental health and substance use problems. Hospitalizations for mental illness are most likely to occur between the ages of 25 and 44 years (32 per cent), which has the potential to disrupt people’s lives during their most productive working years (Canadian Institute for Health Information, 2015).
Mental health and substance use and specific populations
Physical illness and physical disability
The extra pressures that physical disability brings can contribute to mental health and substance use problems. Similarly, the strain of having a long-term physical illness can make people more vulnerable to developing mental health and substance use problems. People living with poor mental well-being are at increased risk of developing a range of physical health problems, including diseases of the immune system and cardiovascular system.
Age/gender
People of all ages can experience poor mental health and/or substance use problems. The way these problems are experienced, as well as their signs and symptoms, is influenced by a person’s age. Some mental health and substance use problems are more common than others at different stages in life.
The onset of many mental illnesses occurs during adolescence and young adulthood. For example, schizophrenia and eating disorders commonly develop from early adolescence through young adulthood. A recent Canadian study reported a high rate of hospitalizations in young people connected to self-inflicted injuries, for young women these rates peaked between ages 15 to 19 years, and for young men in the 20 to 24 age range” (Skinner et al., 2016).
Men and women experience mental health and substance use disorders at different rates and seek different treatments. Women are more likely than men to use health services for a mental illness, especially those between the ages of 25 to 39 years (Public Health Agency of Canada, 2015). Women are 1.5 times more likely to have mood or anxiety-related disorders than men. Men are 2.6 times more likely to be diagnosed with substance use disorders (Minister of Public Works and Government Services Canada, 2006). According to a 2017 profile of Canadians with mental health-related disabilities, women were more likely to report requiring counselling and support group services, while men were more likely to report requiring addiction services (Statistics Canada, 2020).
Sexuality
Members of the 2SLGBTQ+ (two-spirited, lesbian, gay, bisexual, transgendered and transsexual, and questioning) community may encounter a range of difficulties that can contribute to mental health and substance use problems. Although society is becoming more accepting, many 2SLGBTQ+ people still experience feelings of isolation and rejection (Minister of Public Works and Government Services Canada, 2006).
Individuals are more likely to experience higher rates of depression, anxiety, suicidal thoughts and acts, self-harm, and substance use disorders than their heterosexual peers. Meta-analysis studies have found that members of the 2SLGBTQ+ community are 1.5 times more likely to develop depression and anxiety disorders and 2.5 times more likely to attempt suicide (Rainbow Health Ontario, 2012). The high risk for mental health and substance use disorders can be connected to experiences of stigma, prejudice, discrimination, internalized feelings of negativity and expectations of rejection (Gilmour, 2019), as well as interpersonal violence, childhood maltreatment and personal loss (Rainbow Health Ontario, 2012).
Indigenous people
Many factors contribute to the mental health and substance use problems among Indigenous people. Some communities see high rates of mental health and substance use problems and suicide, while others do not. Services available to the general Canadian population do not always reflect the most appropriate approach to healing for respective cultures within Indigenous populations.
Cultural diversity
Racism and discrimination place extra pressures on those from immigrant, refugee, ethnocultural and racialized communities. Language and cultural differences also make it more difficult for people to access appropriate help. Services that are helpful to the general population may not be equally effective for those from different cultural backgrounds, especially if there are language or geographic barriers. Any successful communication recognizes the uniqueness of every culture, relationship and individual. Some forms of verbal and nonverbal communication are appropriate, and others are not. For instance, individuals from some cultures may regard prolonged eye contact as rude. When an individual does not speak English at all, has limited English or chooses to communicate their distress in their primary language, the ideal solution is to use a professional interpreter.
The choice to use a trained interpreter or a family member to interpret must be made by the individual who is experiencing problems. Being able to do so will help the person to feel that they are in control of the situation.
A good interpreter will concentrate on accurately conveying equivalent meaning as well as reporting the direct answers to questions and other responses offered. Everyone has different ways of communicating fears and needs when becoming unwell. If the opportunity is available, exploring the person’s life experiences, value and belief systems, and their reactions to illness, care and support may help establish what is realistic for the individual and what is culturally acceptable.
It is important to recognize both individual and cultural differences. For example, refugees have similar problems to those of settled minority ethnic communities but may face additional challenges if they have experienced torture and political oppression.
Recovery to improved mental well-being
“Recovery” in the context of mental health and substance use problems refers to the lived experiences of people as they accept and overcome the challenge of their problem or disorder. Recovery is much more than achieving the absence of symptoms and means different things to different people.
Recovery has been described as:
“…a way of living a satisfying, hopeful and contributing life even with the limitation caused by illness. Recovery involves the development of new meaning and purpose in one’s life as one grows beyond the catastrophic effects of mental illness” (Anthony, 1993).
Some of the cornerstones of recovery are hope, education, self-advocacy, support, and willingness and responsible action by both the ill person and their helpers (Mental Health Commission of Canada, 2015).
Recovery can progress slowly. Many different factors contribute to recovery, including:
- Having support from family and friends
- Having a meaningful role in society through employment or education opportunities
- Getting professional help early
- Getting the best possible treatments and the person’s willingness and ability to take up the opportunities available.
Mental well-being is everyone’s business. The attitudes and beliefs that society has about mental health and substance use problems have a powerful impact on mental well-being and the recovery of individuals experiencing these problems. Recovery is about supporting each individual’s journey in using their strengths and mental well-being toward living a meaningful life—even with symptoms of mental health and/or substance use problems.
Newer, more effective treatments mean that people with mental health and substance use problems experience fewer side effects and are able to do more while in treatment or recover more quickly and completely. Therefore, a diagnosis of a mental health and/or substance use problem does not mean the same thing for all people at all times. Individuals are encouraged to work closely with their health care providers to get the best results possible.
In addition, some mental health problems are cyclic (such as bipolar disorder), while others can occur in episodes with symptom-free periods in between (such as depression and schizophrenia). For these reasons, it is important at all times that we consider people as individuals, rather than making assumptions based on their diagnosis.
Recovery is about much more than achieving an absence of symptoms. For some people, it can be a long-term process, often described as a journey, and it may not necessarily be a linear process—there may be setbacks along the way.
It is important to recognize that mental health and substance use problems can develop over a long time, and recovery may also take time. The holistic interpretation of recovery found in “Guidelines for a Recovery-Oriented Practice,” primarily developed and promoted internationally by the Mental Health Commission of Canada (MHCC), offers guidelines to help improve understanding about recovery and to promote the application of recovery principles in practice (Mental Health Commission of Canada, 2015).
MHFA Actions

MHFA Actions – ALGES
A
Approach the person, assess and assist with any crisis
L
Listen and communicate nonjudgmentally
G
Give reassurance and information
E
Encourage the person to reach out to supports
S
Self-care for the first aider
Action: Approach the person, assess and assist with any crisis
This action is to approach the person, look out for any crises and assist the person in dealing with them. The key points for the first aider are to:
- Approach the person about their concerns
- Find a suitable time and space where both people feel comfortable
- If the person does not initiate a conversation with the first aider about how they are feeling, the first aider should say something to them
- Respect the person’s privacy and confidentiality.
In a situation involving a person living with a mental health and/or substance use problem, several crises may emerge:
- The person attempts to harm themselves, e.g., by attempting suicide, by using substances to become intoxicated or by engaging in non-suicidal self-injury
- The person experiences extreme distress, e.g., a panic attack, a traumatic event or a severe psychotic state
- The person’s behaviour is very disturbing to others, e.g., they become agitated or lose touch with reality.
If the first aider has concerns that the person is in crisis, the first aider needs to apply crisis first aid (see Section 3).
Action: Listen and communicate nonjudgmentally
Listening and communicating with the person is a very important skill. When listening and communicating, it is important for the first aider to set aside any judgments made about the person or their situation and avoid expressing these judgments. Most people who are experiencing distressing emotions and thoughts want to be listened to empathetically before being offered options and supports that may help them. When listening nonjudgmentally, the first aider needs to adopt certain attitudes and to use verbal and nonverbal communication skills that:
Allow them to really hear and understand what the person is saying, and
Make it easier for the person to feel they can talk freely about their problems without being judged.
It is important to listen and communicate nonjudgmentally at all times when providing MHFA.
Action: Give reassurance and information
Once a person has felt listened to, it can be easier for the first aider to offer support and information. At the time of crisis, the first aider should offer emotional support such as giving the person hope for recovery, empathizing with how they feel, and offering practical help with tasks that may seem overwhelming at the moment. Also, the first aider can ask the person whether they would like some information about mental health and/or substance use problems.
Action: Encourage the person to reach out to supports
A goal of MHFA is to encourage the person to reach out to supports that could help with their recovery to improved mental well-being. You can find resources and links to supports on the Opening Minds Resource hub at: r.openingminds.org. Be prepared to share these when offering MHFA. A person with mental health and/or substance use problems will generally have a better recovery with appropriate professional help. However, they may not know about the various options that are available to them, such as medication, counselling or psychological therapy, support for family members, assistance with vocational and educational goals, and assistance with income and accommodation.
The first aider can also encourage the person to use self-help strategies and to seek the support of family, friends and others. Other people who have experienced mental health and/or substance use problems can also provide valuable help in the person’s recovery.
Action: Self-Care for the first aider
After providing MHFA to a person who is in distress, you may feel worn out, frustrated or even angry. You may also need to deal with the feelings and reactions you set aside during the encounter. It can be helpful to find someone to talk to about what has happened. If you do this, you need to remember to respect the person’s right to privacy. If you talk to someone, don’t share the name of the person you helped or any personal details which might make them identifiable to the person you choose to share with.
It can also be good to do things which improve your own mood or mental well-being. Activities which are known to be helpful for improving mood and reducing anxiety include eating well, keeping regular sleep habits, practicing relaxation techniques such as progressive muscle relaxation, being physically active, talking to supportive people, letting other people know how you are feeling, scheduling enjoyable activities (particularly those that give a sense of achievement), and doing other things you know have been helpful in the past (A. J. Morgan et al., 2012).
Applying MHFA Actions
Section 2 in this guide gives a detailed explanation of how to apply the MHFA actions to a person who may be developing or experiencing a worsening of one or more of the following:
- Depression
- Anxiety problems
- Psychosis
- Substance use problems
- Gambling problems
- Feeding and eating disorders
Section 3 in the guide describes the best ways to assess and assist a person who is experiencing a mental health or substance use crisis. The following crises are covered:
- Suicidal thoughts and behaviours
- Non-suicidal self-injury
- Panic attacks
- Following a traumatic event
- Severe psychotic states
- Severe effects from alcohol use
- Severe effects from drug use
- Agitated behaviours
There are other problems and crises which are not covered in the MHFA course and guide, including personality disorders. However, the skills learned are useful when assisting anyone who is distressed or in crisis, regardless of the underlying problem.
Providing MHFA to diverse cultures and populations
When providing MHFA to a person who is from a culture or population that is different from your own, it is important to:
- Be aware that culture shapes each individual’s understanding of health and ill health
- Learn about specific cultural beliefs that surround mental health and substance use problems in the person’s community
- Learn how these terms are described in the person’s community (i.e., become familiar with the words and ideas used to talk about symptoms or behaviours related to these problems)
- Be aware of taboo concepts, behaviours or language (i.e., learn what might cause shame)
- Do not make assumptions about beliefs, practices or preferences.
This involves:
- Respecting the culture of the community by using the appropriate language and behaviour
- Never doing anything that causes the person to feel shame
- Supporting the person’s right to make decisions about seeking culturally based care.
Providing MHFA to a 2SLGBTQ+ person
Guidelines for communicating with a 2SLGBTQ+ (Two-Spirit person, Lesbian, Gay, Bisexual, Transgender, Transsexual, Queer, Questioning) about mental health and substance use problems are available in the Appendix.
Spectrum of interventions for mental health and substance use problems
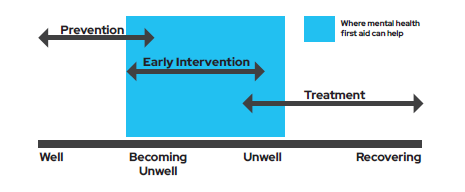
Society has a wide range of interventions for preventing mental health and substance use problems, and for helping people that live with them. MHFA is just one part of the spectrum of intervention. The diagram below illustrates different states of mental well-being, ranging from being well to developing mental health and substance use problems, to having a mental illness and to recovery. There are different types of interventions that are appropriate at these states of mental health and substance use. For the person who is well or has some mild symptoms, prevention programs are appropriate. For the person who is moving from mild mental health and/or substance use problems to a mental illness, early intervention programs such as MHFA can be used. For a person who is very unwell, a range of treatment and support approaches are available, which will assist the person in their recovery process.
Prevention
Prevention programs are available to help everyone in the community, as well as targeted programs for people who are particularly at risk. Examples include parenting skills training, drug education and resilience training programs in schools, promotion of physical exercise to improve mood, stress management courses and policies to reduce stress in the workplace.
Early intervention
Early intervention programs target people living with mental health and/or substance use problems and those who are just developing these problems. They aim to prevent problems from becoming more serious and reduce the likelihood of secondary effects such as loss of employment, school dropout, relationship breakup and drug and alcohol problems. Many people have a long delay between developing a mental illness and receiving appropriate treatment and support. The longer people delay getting help and support, the more difficult their recovery can be.
It is important that people are supported by their family, friends and work colleagues during this time. People are more likely to seek help if someone close to them suggests it (Cusack et al., 2004; Vogel et al., 2007). It is during this early intervention phase that helping with MHFA actions can play an important role.
Treatment and supports
There are many different types of treatment and supports that can help people in their recovery to improved mental well-being. Once the person has made the decision to seek help, they may choose from a number of sources of help, treatment approaches and service settings. There is no “one-size-fits-all” approach.
Medical Treatments
These include various types of prescribed medications and other treatments given by a family physician.
Psychological treatments
Psychological treatments provide a supportive relationship and seek to change the way the person thinks or behaves. Usually, treatment involves talking individually, or sometimes in a group, with a mental health or addictions professional to address issues and to promote personal growth and coping skills. Self-help books and computerized psychological treatments are also available.
Complementary treatment and lifestyle changes
These involve using natural or alternative therapies and changing the way one lives. These can be used under the guidance of a health professional or as self-help. Care should be taken to ensure that the self-help strategies employed are evidence based or have been recommended by an appropriate professional.
Support groups
These groups bring people with common problems together to share experiences and help each other. Participation in mutual-aid self-help groups can help reduce feelings of isolation, increase knowledge, enhance coping skills and bolster self-esteem.
Rehabilitation programs
These programs help people regain skills and confidence to live and work in their community.
Family and friends
Family and friends are a very important source of support for recovery to improved mental well-being. Family and friends can help by having an understanding of the problem and providing the same support as they would if the person has a physical illness.
MHFA can continue to play an important role in this period if relapses or crises occur. At such times, people need to be supported by those around them, in particular when no expert help is immediately available.
Professionals who can help
A variety of health professionals can help people to improve their mental well-being:
Family physicians
For many people developing a mental health and/or substance use problem, their family physician will be the professional they first turn to for help. A family physician can recognize symptoms and provide the following types of help:
- Look for a possible physical cause
- Explain the problem and how the person can best be helped
- Prescribe medication if needed
- Refer the person to a psychologist or allied health professional who can help the person learn ways to cope with and overcome the illness
- Refer the person to a psychiatrist, particularly if the symptoms are severe or long lasting
- Link the person to community supports.
Psychologists
A psychologist is someone who has studied human behaviour at university and has had supervised professional experience in the area. Psychologists are registered with a national registration board. Some psychologists provide treatment to people with mental illnesses. Psychologists do not have a medical degree, so they do not prescribe medication. Some psychologists work for health services, while others are private practitioners.
A clinical psychologist is a psychologist who has undergone additional specialist training in how to treat people with mental health and/or substance use problems. They are particularly skilled at providing cognitive behaviour therapy and other psychological treatments.
Psychiatrists
Psychiatrists are medical doctors who specialize in the treatment of mental health and/or substance use problems. Psychiatrists mostly focus on treating people with severe or long-lasting problems. They are experts in medication and can help people who are having side effects from their medication or interactions with other medications. It is possible to see a psychiatrist by getting a referral from a family physician. A family physician might refer a patient to a psychiatrist if they are very ill or are not getting better quickly. Most psychiatrists work in private practice, but some work in clinics or hospitals.
Mental health and substance use nurses
Mental health and substance use nurses are registered nurses who are specialized in caring for people with mental illnesses. They generally care for people with more severe illnesses who are treated in hospitals or in the community. They can provide assistance with medication, practical support and counselling.
Occupational therapists and social workers
Most occupational therapists and social workers work in health or welfare services. However, some have additional training in mental health and substance use and are registered by Medicare. They can provide treatments similar to psychologists.
Counsellors
Counsellors can provide psychological support. However, counsellors are not a profession registered by the government, so anyone, even those without qualifications, can call themselves a “counsellor.” A well-qualified counsellor may also be a psychologist or other registered professional. Some counsellors may have specific training and skills in an area such as drug and alcohol counselling.
Supports — Opening Minds Resource Hub
A key part of the role of a mental health first aider to to encourage the person we are helping to reach out to supports that can help with recovery to improved mental well-being. A list of these supports is available on the Opening Minds (OM) Resource Hub. This hub includes resources to support someone who needs it as well as information for first aiders themselves about mental health, resiliency, and supporting others. It includes national and provincial supports, academic articles, and links to external information that be of interest as you continue learning. Please go to this hub and familiarize yourself with the list of supports in preparation to share these with people you offer MHFA to.
Go to: r.openingminds.org